
Nearly four decades ago, dietary fat was deemed unhealthy. Reductionist scientific views implicated fat as the sole macronutrient contributing to heart disease. We adopted the belief that “calories in vs. calories out” was superior to food choice and quality, and accepted the dogmatic view that eating dietary fat, creates more adiposity (body fat).
In the 1980’s The U.S. Dietary guidelines exemplified a push towards low fat, high carbohydrate containing foods including: cereals, breads, pastas, lean poultry and low-fat dairy. These guidelines warned us to limit total fat consumption and recurrent literature influenced nutrition education, policy, and food buying and consumption patterns. We began avoiding fat containing foods such as egg yolks, red meat, avocados, and butter.
Following a long lasting “low fat” nutrition movement, the pendulum swung, this time prompted by low carbohydrate programs such as Atkins, Ancestral eating, Whole 30, and the Paleo movement. Such protocols have directed individuals to increase fat consumption, use liberal amounts of coconut oil, butter, and bacon, and restrict otherwise healthy foods including legumes, fruits and starchy vegetables. We now sit somewhere in between two dietary extremes.
The truth is, the amount of saturated fat acceptable in a healthy diet is still up for debate. All fats are not created equal, saturated fats are not monolithic, & the source of dietary fat is considerably more important than ever.
Here’s what you need to know:
As of 2015, The Dietary Guidelines Advisory Committee concluded that low-fat diets have no effect on cardiovascular disease and emphasized the importance of healthful, food-based dietary patterns. Also in 2015, the FDA stated trans fats are no longer generally recognized as safe (GRAS).
The best way to consume healthy fats is through the selection of foods naturally rich in fat. Here’s our view:
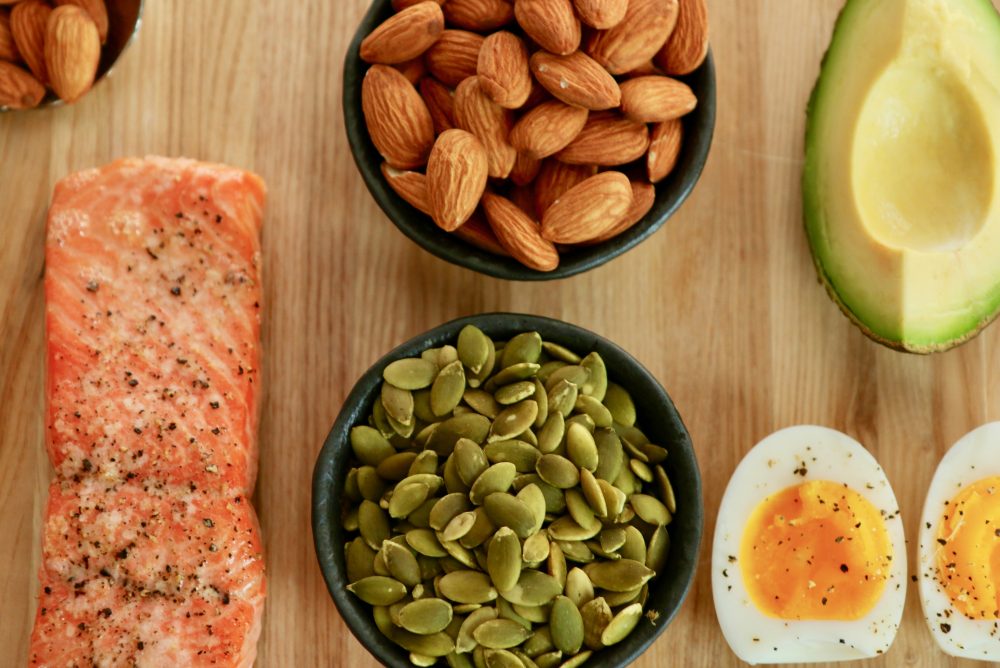
Monounsaturated fats improve blood pressure and cholesterol through lowering LDL cholesterol, lowering blood clotting factors, aiding with inflammation, and improving glucose. Monounsaturated fatty acids have been shown to improve glucose tolerance and other risk factors contributing to metabolic syndrome. We suggest focusing on whole food sources rich in monounsaturated fats. These include: Extra Virgin Olive Oil (cold pressed at room temperature), raw almonds, cashews, pecans, peanuts, avocados, natural nut butters, sesame seeds, and olives.
Omega-3 fatty acids are vital to the formation of cell membranes and hormone production. Research shows regular consumption of Omega-3 fatty acids minimize the risk of heart attack and stroke. In addition, Omega-3 fatty acids decrease inflammation, protect against cognitive decline, and lower blood pressure. Since we cannot make Omega-3 fatty acids in our bodies, we must rely on food sources to achieve optimal health.
Interestingly, omega-6 and omega-3 fatty acids compete for biosynthetic enzymes. Because the Western diet is inundated with processed foods and copious amounts of vegetable oil, the ratio of omega-6 fatty acid consumption to omega-3 fatty acid consumption is nearly to 20:1. Simply put, we are eating way too many omega-6 fatty acids.
Here’s the takeaway! The body needs omega-3 fatty acids from both plant and animal sources: (ALA, EPA and DHA respectively.) The best foods to consume include: wild fish, grass fed/pasture raised meats, wild plants, flax, pumpkin and chia seeds.
Look for hidden omega-6 fatty acid sources such as vegetable oil, margarine, & processed foods containing soybean oil, and canola oil. Check your “healthy” pantry staples & refrigerator condiments (enter: hummus, grain-free chips, red pepper sauce etc.)
A trans fat is a polyunsaturated or monounsaturated fatty acid with a double bond in the “trans” position rather than the cis position. Trans fats and partially hydrogenated oils are most often hidden as food additives. Don’t be fooled! These ingredients have clear adverse effects.
Here’s the takeaway! Nature doesn’t produce unhealthy fat. Eat fat sources from whole foods, forgo isolating macronutrients, and limit hydrogenated fats as a food ingredients.
Can you recall the last time you had a full blood work panel? Have you discussed cholesterol, blood pressure, and blood sugar numbers with your physician? We suggest initiating a conversation with the doctor to understand baseline values.
xx,
WeCollab
Resources:
Mayo Clinic Nutrition and Healthy Eating
Mozaffarian, D. (2016). Dietary and Policy Priorities for Cardiovascular Disease, Diabetes, and Obesity – A Comprehensive Review. Circulation, 133(2), 187–225.
Schwingshackl, L., & Hoffmann, G. (2014). Monounsaturated fatty acids, olive oil and health status: a systematic review and meta-analysis of cohort studies. Lipids in Health and Disease, 13, 154.
Simopoulos, A. P. (2016). An Increase in the Omega-6/Omega-3 Fatty Acid Ratio Increases the Risk for Obesity. Nutrients, 8(3), 128.
Qian, F., Korat, A. A., Malik, V., & Hu, F. B. (2016). Metabolic Effects of Monounsaturated Fatty Acid–Enriched Diets Compared With Carbohydrate or Polyunsaturated Fatty Acid–Enriched Diets in Patients With Type 2 Diabetes: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Diabetes Care, 39(8), 1448–1457.
Qi Sun, Jing Ma, Hannia Campos, Kathryn M Rexrode, Christine M Albert, Dariush Mozaffarian, Frank B Hu; Blood concentrations of individual long-chain n–3 fatty acids and risk of nonfatal myocardial infarction. The American Journal of Clinical Nutrition, Volume 88, Issue 1, 1 July 2008, Pages 216–223.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}